Scoliosis is estimated to affect 4.5% of the general population. In the United State of approximately 273 million people, this means that over 12 million cases of scoliosis exist, and almost 500 more are diagnosed every day – about 173,000 every year! According to some studies, the average scoliosis patient will suffer a 14-year reduction in their average life expectancy. This means that if by some miracle we could eliminate scoliosis completely; this would add 168 million years of health and productivity to our society. Clearly this is not a minor issue, but an epidemic, and one that should be taken very seriously
Scoliosis affects 5 to 7 million people in North America. More than a half million visits are made to doctors’ offices each year for evaluation and treatment of scoliosis. Although scoliosis can begin at any age, it most often develops in adolescents between the ages of 10 and 15. Girls are more commonly affected than boys. Because scoliosis can be inherited, children whose parents or siblings are affected by it should definitely be evaluated by a trained professional.
Click here for infographic, “Scoliosis by The Numbers”
Scoliosis is diagnosed in a very specific manner. Typically, the doctor will obtain a family history, since scoliosis has shown a significant genetic link. Chances are, if your child has scoliosis, a sister, brother, parent, or grandparent also has it to some degree. Once you family history is taken, certain orthopedic tests are conducted, such as an Adam’s forward bending test. This test shows if there is a rib hump present on one side of the spine. The only true objective means, however, for determining if your child has scoliosis is by taking spinal x-rays. The scoliosis is measured at the top and bottom of the curvature by a geometrical measurement called Cobb’s angle. Conventional medicine proposes that a scoliosis below 20° typically does not need to be treated, especially if there are no symptoms present.
Every year in the US, roughly 20,000 Harrington rod implantation surgeries are performed on patients with scoliosis, at an average cost of $120,000 per operation. Each year 8,000 people who underwent the surgery are legally defined as permanently disabled.
Follow up x-rays on these individuals show that about 22 years after surgery their scoliosis has returned to pre-surgery levels. The Harrington rods bend, break loose from the wires, or worse break completely in two. Corrosion (rust) is also found in two out of every three Harrington rod patients. After the operation, the average patient also suffers a 25% reduction in their spinal range of motion.
Please do not have surgery before investigating our methods and discussing your case with us!
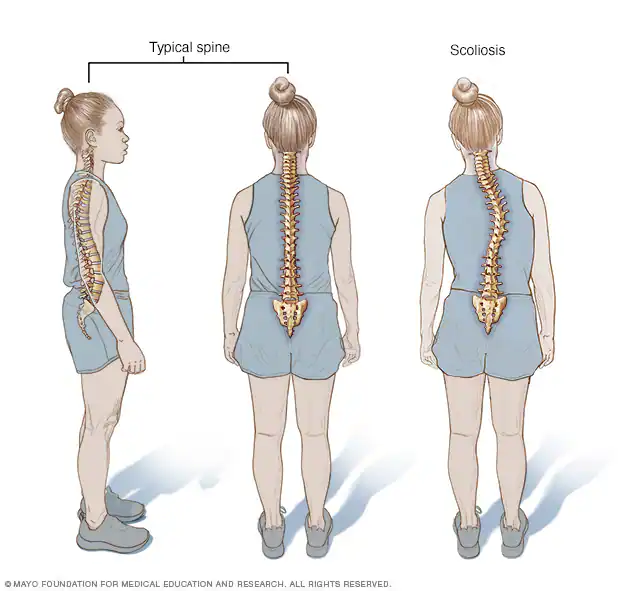
What is scoliosis?
Because we walk on 2 feet, the human nervous system constantly works through reflexes and postural control to keep our spine in a straight line from side to side and front to back. Occasionally, a lateral (sideways) curvature develops. If the curvature is larger than 10 degrees, it is called ‘scoliosis’. Curves less than 10 degrees are often just postural changes possibly as a result of muscular imbalances. Scoliosis can also be accompanied by lordosis (abnormal curvature toward the front) or kyphosis (abnormal curvature toward the back). In most cases, the vertebrae are also rotated.
In more than 80% of cases, the cause of scoliotic curvatures is unknown; we call this condition ‘idiopathic’ scoliosis. In other cases, trauma, neurological disease, tumors, and the like are responsible. Functional scoliosis is often caused by some postural problem, muscle spasm, or leg-length inequality, which can often be addressed. Structural scoliosis does not reduce with postural maneuvers. Either type can be idiopathic or have an underlying cause. Scoliosis is an abnormal sideways curvature of the spine that affects 2 to 4% of the population. This condition usually goes unnoticed, especially as it rarely causes problems in the early years. It can begin in infancy, childhood or adulthood, but is usually seen in adolescents.
Click here for video, “What is Scoliosis?”
Although this condition can occur in both males and females, it is about ten times more common in females. The scoliosis curvature is often shaped like the letter ‘S’ or ‘C’… and the spine is sometimes also twisted. Parents may see an uneven waist or shoulders, particularly prominent shoulder blades or shoulders, elevated hips or leaning to one side. The rib cage can also become more prominent on one side, this becomes more evident if you ask the person to bend forward while observing them from behind.
Click here for video “Scoliosis Pain and Chiropractic”
What Causes Scoliosis?
In some cases, the scoliosis is caused by underlying factors that can be treated. For example:
– back pain – muscle spasm – differing leg lengths – osteoarthritis – osteoporosis – appendicitis
These factors may cause the spine to become curved and may be reversed.
What are the symptoms of scoliosis?
Scoliosis can significantly affect the quality of life by limiting activity, causing pain, reducing lung function, or affecting heart function. Diminished self-esteem and other psychological problems are also seen. Because scoliosis occurs most commonly during adolescence, teens with extreme spinal deviations from the norm are often teased by their peers.
Fortunately, 4 out of 5 people with scoliosis have curves of less than 20 degrees, which are usually not detectable to the untrained eye. These small curves are typically no cause for great concern, provided there are no signs of further progression. In growing children and adolescents, however, mild curvatures can worsen quite rapidly—by 10 degrees or more—in a few months. Therefore, frequent checkups are often necessary for this age group.
General Types of Scoliosis
As the spine improperly twists and bends, the nerves emitting between the vertebrae (spinal bones) have the potential for being compressed and irritated. Once irritated, these nerves will lead to abnormal function in the organ that they control.
There are two general types of scoliosis, a structural scoliosis and a functional scoliosis.
The structural type is due to an improperly formed bone. The bone may have been malformed by a birth defect, or may have developed from a fractured bone which healed with an abnormal shape. Since gravity is always pulling down on the body, the structure which is resting on top of the malformed bone may not sit level. This is the beginning of a tilt to the spine.
Functional scoliosis, the most common type, is due to the tilting of an intervertebral disc (the shock absorber) between the vertebrae. The functional scoliosis is usually due to some type of spinal injury. Such an injury may be obvious like a physical trauma, or may not be so obvious, like carrying a heavy book bag over one shoulder.
Idiopathic Scoliosis
About 80 percent of scoliosis cases are idiopathic, meaning the cause is unknown. There is no research evidence that chiropractic treatment can “cure” idiopathic scoliosis. But our treatment can help give relief for some of the pain caused by idiopathic scoliosis. That will help your child to stay active which is important for their general health and well-being.
Scoliosis can run in families. A child who has a parent, brother, or sister with idiopathic scoliosis should have regular check-ups. Adults who had scoliosis as children are more likely to have chronic back pain than people in the general population. Therefore, the most important thing is to detect the scoliosis in the first place, diagnose the cause of the scoliosis and then treat it appropriately.
Chiropractic care maintains the mobility of the joints of the spine and allows the spine to develop normally. Proper treatment, especially if commenced earlier than later, can prevent progression of the curve and may help reduce it. With scoliosis particularly, an ounce of prevention is worth a pound of cure.
Common Physiological Effects of Idiopathic Scoliosis on the Body:
NEUROLOGICAL EFFECTS
OSSEOUS EFFECTS
BIOMECHANICAL EFFECTS
MUSCULAR EFFECTS
BIOCHEMICAL EFFECTS
NEUROLOGICAL EFFECTS
Due to the compensatory head tilt, the orbits of the eyes in a scoliotic patient are unleveled. This unleveling in turn affects the balance mechanism, proprioception and oculo-vestibular function of the patient. The spinal cord is subjected to lateral deviation and the dorsal nerves are stretched in some areas and atrophied in other areas. Research shows that a 10% stretch applied to a nerve will affect the nerves ability to transmit impulses.
OSSEOUS EFFECTS
The most obvious aspect of this disease is the impact upon the spine itself. The vertebral bodies of the spine are subjected to abnormal pressures due to the distortion, which is developing. This may result in asymmetry in the individual vertebra. Interestingly, the vertebral bodies of the scoliotic patient are 50% taller and 15% wider than average.
BIOMECHANICAL EFFECTS
Scoliotic patients have hyperflexibility in the ligaments which hold the spine and this hyperflexibility contributes to the three dimensional distortion which occurs. The spine becomes laterally curved as well as rotated. This distortion negatively impacts the discs between the vertebra and causes fibrous changes to the ligaments.
MUSCULAR EFFECTS
The muscles that attach to the spine directly are greatly affected due to the curvature. As the origins and insertions of the muscles are contorted due to changes in the force vectors caused by the curvature, the muscles can begin to work against the patient. Ultimately, these compromised muscles add to the problem. With time the muscles also begin to develop scar tissue.
BIOCHEMICAL EFFECTS
Patients with Idiopathic Scoliosis also have nutritional challenges, which must be addressed. There is reason to believe that the scoliotic patient has digestion and absorption problems. They tend to have compromised immune systems leaving them subject to flu and viruses. These patients harbor some unusual and often extreme mineral imbalances as demonstrated by hair mineral analysis. These nutritional imbalances contribute to the hormonal imbalances which ultimately contribute to the ligamentous laxity which accelerates the condition.
How is scoliosis evaluated?
Evaluation begins with a thorough history and physical examination, including postural analysis. If a scoliotic curvature is discovered, a more in-depth evaluation is needed. This might include a search for birth defects, trauma, and other factors that can cause structural curves.
Patients with substantial spinal curvatures very often require an x-ray evaluation of the spine. The procedure helps determine the location and magnitude of the scoliosis, along with an underlying cause not evident on physical examination, other associated curvatures, and the health of other organ systems that might be affected by the scoliosis. In addition, x-rays of the wrist are often performed. These films help determine the skeletal age of the person, to see if it matches an accepted standard, which helps the doctor determine the likelihood of progression. Depending on the scoliosis severity, x-rays may need to be repeated as often as every 3 to 4 months to as little as once every few years.
Other tests, including evaluation by a Scoliometer™, might also be ordered by the doctor. This device measures the size, by angle, of the rib hump associated with the scoliosis. It is non-invasive, painless, and requires no special procedures. A Scoliometer™ is best used as a guide concerning progression in a person with a known scoliosis—not as a screening device.
Home Test for Childhood Scoliosis
Here is a home test for childhood scoliosis (courtesy of Dr. Fred Barge, Chiropractor, from his text “Scoliosis”) that may aid in the early detection of scoliosis. Have the child strip to the waist and observe her/his posture from behind:
Does the child hold their head tipped to one side?
Is one shoulder higher than the other?
With both arms hanging down to their side, is there more room between their body and an arm on one side or the other?
Looking at the child’s waist, does one side curve in more than the other?
Does one hip appear prominent than the other?
Have the child bend over at the waist (as to touch their toes). Does one side of the spine appear more prominent than the other? Is there a hump on one side between the shoulders or on the lower back?
If any of the above tests appear positive, then have your child checked by a chiropractor for scoliosis.
Chiropractors use medical and family history, physical and neurological examination when checking a person for scoliosis. An X-ray will help to diagnose the scoliosis and lets the chiropractor measure the curve and see its location, shape and pattern. An early X-ray is useful to check for any subsequent increase in curvature later on.
Idiopathic scoliosis
Despite years of research doctors don’t know what causes the most common type of scoliosis. When a cause can’t be identified, the scoliosis is called idiopathic scoliosis.
Most cases develop in children between the ages of 9 and 14 during the growth spurt of puberty. It affects more girls than boys with 80 percent of adolescent cases affecting girls.
As the curvature gets worse, the spine tends to rotate. This can affect the ribs, which become prominent on one side.
In severe cases of early onset upper back scoliosis, the rotated ribs may limit the amount of air getting to the lungs and putting strain on the heart. This increases the risk of heart failure.
This is why early diagnosis is important – appropriate treatment can prevent serious complications.
What is the treatment for scoliosis?
There are generally three treatment options for scoliosis—careful observation, bracing, and surgery. Careful observation is the most common “treatment,” as most mild scolioses do not progress and cause few, if any, physical problems. Bracing is generally reserved for children who have not reached skeletal maturity (the time when the skeleton stops growing), and who have curves between 25 and 45 degrees. Surgery is generally used in the few cases where the curves are greater than 45 degrees and progressive, and/or when the scoliosis may affect the function of the heart, lungs, or other vital organs.
Chiropractic spinal manipulation, therapeutic exercise and electrical muscle stimulation have also been advocated in the treatment of scoliosis. None of these therapies alone has been shown to consistently reduce scoliosis or to make the curvatures worse. For patients with back pain along with the scoliosis, manipulation and exercise may be of help.
Most people with scoliosis lead normal, happy, and productive lives. Physical activity including exercise is generally well-tolerated and should be encouraged in most cases.
Is scoliosis always progressive?
Generally, it is not. In fact, the vast majority of scolioses remains mild, is not progressive, and requires little treatment, if any.
In one group of patients, however, scoliosis is often more progressive. This group is made up of young girls who have scolioses of 25 degrees or larger, but who have not yet had their first menstrual period. Girls generally grow quite quickly during the 12 months before their first period and if they have scolioses, the curvatures tend to progress rapidly. In girls who have already had their first periods, the rate of growth is slower, so their curves tend to progress more slowly.
Call Advanced Healthcare today at (758) 518-5000 and have Dr. Isidore evaluate you or your child to determine if spinal scoliosis is demonstrated, and recommend appropriate treatment options.
References:
Clinically Oriented Anatomy, 2nd Edition, Kieth L. Moore, Ph.D., F.I.A.C., Williams & Wilkens, 1985. Pgs 568-569.
Principles of Anatomy and Physiology, 6th Edition, Gerald J. Tortora & Nicholas P. Anagnostakos, Harper & Row, 1990. Pg. 187
Textbook of Clinical Chiropractic: A Specific Biomechanical Approach., Gregory Plaugher, editor. Williams and Wilkens 1993, Pgs 266-278.
Fundamentals of Orthopedics, 3rd Edition. John J. Gartland, M.D. , W.B. Saunders Company 1979. Pgs.339-343.
Rothman, R., M.D., Simone, M.D., The Spine, 3rd edition W.B. Saunders Company, 1992.
Bradford, D., M.D., Lonstein, M.D., Textbook of Scoliosis and Other Spinal Deformities, 3rd edition, W.B. Saunders Company, 1994.
Kein, H., The Adolescent Spine, 2nd edition, Springer-Verlag, 1982.
Cailliet, Rene, M.D., Scoliosis: Diagnosis and Management, F.A. Davis, 1975.
Dingle, R.V., (ed.), The CIBA Collection of Medical Illustrations; Vol. 8, Musculoskeletal System; Part II Developments/Disorder, Tumors, Rheumatic Disease, and Replacement, Summit, NJ, CIBA-Geig Corp:31-36, 1990.
Sallahian, C., Reduction of a Scoliosis in an Adult Male Utilizing Specific Chiropractic Spinal Manipulation: A Case Report, Journal of Chiropractic Research and Clinical Investigation, Vol. 7, No. 2, July, 1991.
Cox, J., Low Back Pain
The American Chiropractic Association
About Scoliosis
Scoliosis Statistics
Spinecor viideo
Spinecor
SPINECOR PROVIDER
About Scoliosis
More recent research has shown the long- term effects of scoliosis may include early arthritis, disc disease, chronic muscle and spine pain, and cardiovascular dysfunction. Additionally, new evidence suggests that people with scoliosis may in fact be in a state of constant pain. Their bodies simply adapt to the presence of a constant low threshold pain syndrome. Bracing, such as the Boston brace, is usually performed on scoliosis curvatures up to 30-45°. However, the purpose of most types of braces is only to halt scoliosis progression, not reverse it. Bracing has been shown, in some cases, to slow the progression of large curvatures over 30 degrees, but has a limited or no effect in the long-term progression of the disease. When a scoliosis progresses beyond 45-50°, surgery becomes the usual prescribed conventional option. Surgery can consist of several techniques, either alone or in combination. Scoliosis surgery does work on a short-term basis, but lifelong follow-ups do not show sustained improvement. In some cases, the surgery has to be repeated when the implanted hardware fails or breaks.
Scoliosis Statistics
Here are some startling statistics about scoliosis:
87% of children ages 3-10 who are diagnosed with scoliosis will undergo surgery to correct the scoliosis. Of these, 20 – 45% will require additional surgeries.
Girls ages 10-16 are 8-10 times more likely to have their scoliosis get worse than boys the same age.
The average adolescent scoliosis (above 30°) worsens by about 7° each passing year.
You don’t have to let your child or loved one become a statistic. There is something you can do about it that works.
Spinecor viideo
To learn about how scoliosis can be treated by a minimally-invasive spinal technique, read the articles below: Introduction to Scoliosis Booklet
by Dr. Clayton Stitzel, D.C.
The Pettibon System: A Neurophysiologic Approach to Spine and Posture Correction
by Mark Morningstar, D.C., Burl R. Pettibon, D.C., and Carol L. Renz, PhD. Chapter in the recently published medical textbook, “Mimimally Invasive Spinal Technique.”
Scoliosis Treatment Using a Combination of Manipulative and Rehabilitative Therapy: A Retrospective Case Series
by Mark W. Morningstar, Dennis Woggon, and Gary Lawrence
Spinecor
SpineCor was developed, with the support of the Canadian government, by two renowned orthopedic surgeons, for the purpose of helping children avoid scoliosis surgery. Since then, it has displayed a 20-year track record in the scientific literature; as well as clinical case studies of tremendously helping many adolescents permanently stabilize and reduce their curves.
Additionally, as of late, the SpineCor brace is successfully being adapted for adults to provide much needed pain relief and support. Adult studies have shown that 90% of adult patients report pain relief within the first 6 weeks.
To-date, SpineCor has been used in at least 20 countries for well over 10,000 patients, by chiropractors, orthopedists, and other healthcare providers.
SpineCor is the ONLY flexible, dynamic bracing system in use, anywhere in the world today. All other scoliosis braces are rigid, hard-shells. Studies have shown that rigid bracing causes muscle weakness and eventual curve progression in the majority of cases.
The SpineCor brace is designed to balance and strengthen the spinal musculature, optimize spinal loading, and retrain neurological feedback. In this manner, the brace isn’t FORCING the spine straighter. It’s RETRAINING THE BRAIN to activate the muscles necessary for the body to correct itself.
If you need more information about the SpineCor Scoliosis Brace Dynamic Spine Center is here to help.
Dr. Charles Isidore is the ONLY doctor on Island certified to provide the SpineCor bracing system.
SpineCor was developed, with the support of the Canadian government, by two reknowned orthopedic surgeons, for the purpose of helping children avoid scoliosis surgery. Since then, it has displayed a 20+-year track record in the scientific literature; as well as clinical case studies of tremendously helping many adolescents permanently stabilize and reduce their curves.
Additionally, as of late, the SpineCor brace is successfully being adapted for adults to provide much needed pain relief and support. Adult studies have shown that 90% of adult patients report pain relief within the first 6 weeks.
To-date, SpineCor has been used in at least 20 countries for well over 10,000 patients, by chiropractors, orthopedists, and other healthcare providers.
SpineCor is the ONLY flexible, dynamic bracing system in use, anywhere in the world today. All other scoliosis braces are rigid, hard-shells. Studies have shown that rigid bracing causes muscle weakness and eventual curve progression in the majority of cases.
The SpineCor brace is designed to balance and strengthen the spinal musculature, optimize spinal loading, and retrain neurological feedback. In this manner, the brace isn’t FORCING the spine straighter. It’s RETRAINING THE BRAIN to activate the muscles necessary for the body to correct itself.
If you need more information about the SpineCor Scoliosis Brace , Dr. Isidore at Dynamic Spine Center is the only Eastern Caribbean SpineCor provider certified by Scoliosis Specialists, can provide it to you. Please call (758) 518-5000