



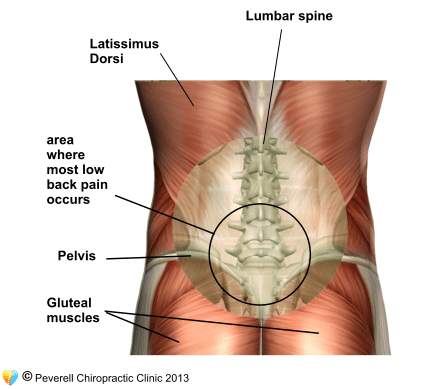
Low Back Pain
Back pain has been found to be one of the most debilitating disabilities worldwide, and most of us may get it at some point in our life. Pain during sitting and sleeping, difficulty walking for a long time, or difficulty bending forwards to play with your kids are common complaints. This pain is definitely limiting and disruptive to your daily routine, taking away your concentration and productivity, making it hard to focus on your work ahead.
Common causes:
LUMBAR DISC INJURY (Common recovery time: 4-12 weeks)
In between our spine, we have discs that are filled with jelly-like fluid. Think of it like a water balloon, when these discs are pressured due to prolonged sitting or lifting, it may press onto the nerves nearby and cause pain at the low back, or even symptoms down towards your legs. In some cases, there could be tears in our discs that can cause intense pain and limitation.


MECHANICAL LOW BACK PAIN (Common recovery time: 2-6 weeks)
Other than spinal discs, we also have other structures like muscle and ligament to support and stabilise our spine. It is common to have muscle or ligament injury as a result of our daily activities such as lifting and carrying.
SACROILIAC JOINT DYSFUNCTION (Common recovery time: 2-8 weeks)
Sacroiliac joint (SIJ) is an important weight bearing joint and plays an important role in distributing weight evenly around our body. When you sit for prolonged hours, this may cause the structures around SIJ to be stiff and lead to the discomfort that you may be having.
 What kind of treatments can help solve back pain?
What kind of treatments can help solve back pain?
- Chiropractic adjustments: Targeted spinal adjustments can be done to reduce stiffness, as well as reduce the pressure on your spine or hip bones, and reduce your pain!
- Physiotherapy rehabilitation: Specific rehabilitative exercises to activate and strengthen the muscles around your back and core to stabilise the spine, teaching you how to manage your pain so you do not need to rely on us! If the injury is fresh, here are some things we would do for you.
- Decompression therapy: In cases where the disc and nerves are involved, a gentle stretching using our one-of-a-kind machine helps to reduce the pressure placed on the neck and improve numbness, tingling, and radiating pain down the arm.
Is there anything I can do at home?
- ICE: Wrap an ice pack, or a bag of ice in a damp towel, over the area of pain for about 15 mins. Ice helps in reducing inflammation and pain.
- Move Around: once then pain has come down a little. Notice if there is any sharp pain or pain traveling down your legs, or if you’re able to move a little better.
- Stand Up: If your job requires you to be sitting at your desk for long hours at a stretch, try standing up, walking a little every hour or so, keep moving even while you’re at the desk. Our body is not meant to stay in one position for long periods of time!
If your pain is still not getting any better, please seek help from a healthcare professional who can give you accurate and targeted advice to help reduce your pain and get you active again!
The most common complaints we hear involve cases of what is reported as “neck pain” or “lower back pain.” In fact, around 80% of all adults will suffer from one of these two ailments at some point in their lifetime.
Back pain is:
- The leading cause of disability in men over 45
- The second most common reason for visits to a primary care physician
- The third most frequent reason for surgical procedures
Back pain varies across the board. For some, it comes on slowly, while others complain of a sudden onset or a “throwing out” of their back. Once it presents itself, the pain may be intermittent or constant. It may feel like a sharp stabbing pain or like a low, dull, ache.
The good news is that in most instances, back pain actually resolves itself in just a matter of weeks – and often without any treatment at all. In some cases, conservative, nonsurgical treatments are used to relieve pain. But for the most part, surgery is not required.
Could I Have a Spine Condition?
Depending on the underlying condition causing your neck or lower back pain, a variety of other associated symptoms may present themselves. If the issue originates in the spine, symptoms may include:
- Pain that extends into the buttocks and legs
- Numbness and tingling (in the hands and feet)
- Pain that is worse when bending
- Trouble with finger coordination
- Weakness or balance problems
In order to answer the question, “Could I have a spine condition?” we encourage you to set up an appointment with a qualified spine physician to be evaluated.
When pain inhibits your ability to turn, bend, stretch or perform other everyday movements, it is time to see a spine specialist to identify the root cause of your pain and to discuss possible treatment options.
Answering the Question on Your Mind
When you see a spine physician, they will perform a thorough physical examination and review your entire medical history, asking you many questions about the nature of your symptoms. In many cases, this initial evaluation may be enough to diagnose the issue, but if your doctor needs more information in order to answer the question, “Could I have a spine condition?” then they will order one or more of the following tests.
- X-ray or CAT scan: An x-ray will show some of the most obvious causes of back pain, such as broken bones and deformities in the spinal curve. For a more detailed look at potential bone problems, a computerized axial tomography (CAT) scan may be requested. This serves as a sort of 3D x-ray.
- MRI: In order to look at possible issues related to muscles, nerves and discs, a magnetic resonance imaging test may be used.
- Bone Scan: If your physician suspects (or wants to rule out) a more rare condition, such as cancer or infection, they will evaluate you with a bone scan.
- Bone Density Test: Osteoarthritis (especially common in the elderly) is one of the most frequently observed causes of spinal fractures. A bone density test will reveal whether your spine has succumbed to the onset of this condition.
Possible Spine Conditions
If you suspect that a spinal condition is causing your back or neck pain, it may be time to research some specific conditions to find out if your symptoms match up. Below are a list of some of the most common spine problems that bring patients in to see a Chiropractor or spine specialists:
· Herniated Cervical Disc · Herniated Lumbar Disc · Spinal Cord Injuries · Spondylosis · Spinal Tumors · Sciatica | · Spinal Infections · Spinal Osteoarthritis (Spondylosis) · Spinal Stenosis · Scoliosis and Spinal Deformities · Whiplash |
Conditions
Research has demonstrated that chiropractic care is a safe and effective way to manage back pain. Whether the pain is due to subluxations (stuck or dysfunctional joints), degenerated joint disease, arthritis, strained muscles, sprained ligaments, herniated disks or flat feet, your chiropractor can help relieve the discomfort associated with the condition.
Clinical Effectiveness and Efficacy of Chiropractic Spinal Manipulation for Spine Pain
Carlos Gevers-Montoro1,2,3 Benjamin Provencher1,2 Martin Descarreaux1,4 Arantxa Ortega de Mues3 Mathieu Piché1,2*
Spine pain is a highly prevalent condition affecting over 11% of the world’s population. It is the single leading cause of activity limitation and ranks fourth in years lost to disability globally, representing a significant personal, social, and economic burden. For the vast majority of patients with back and neck pain, a specific pathology cannot be identified as the cause for their pain, which is then labeled as non-specific. In a growing proportion of these cases, pain persists beyond 3 months and is referred to as chronic primary back or neck pain.
To decrease the global burden of spine pain, current data suggest that a conservative approach may be preferable. One of the conservative management options available is Chiropractic Adjustment, the main intervention used by chiropractors and other manual therapists. The aim of this narrative review is to highlight the most relevant and up-to-date evidence on the effectiveness (as it compares to other interventions in more pragmatic settings) and efficacy (as it compares to inactive controls under highly controlled conditions) of CHIROPRACTIC ADJUSTMENT for the management of neck pain and low back pain. Additionally, a perspective on the current recommendations on CHIROPRACTIC ADJUSTMENT for spine pain and the needs for future research will be provided.
In summary, CHIROPRACTIC ADJUSTMENT may be as effective as other recommended therapies for the management of non-specific and chronic primary spine pain, including standard medical care or physical therapy. Currently, CHIROPRACTIC ADJUSTMENT is recommended in combination with exercise for neck pain as part of a multimodal approach. It is recommended as a frontline intervention for low back pain. Despite some remaining discrepancies, current clinical practice guidelines almost universally recommend the use of CHIROPRACTIC ADJUSTMENT for spine pain. Due to the low quality of evidence, the efficacy of CHIROPRACTIC ADJUSTMENT compared with a placebo or no treatment remains uncertain. Therefore, future research is needed to clarify the specific effects of CHIROPRACTIC ADJUSTMENT to further validate this intervention. In addition, factors that predict these effects remain to be determined to target patients who are more likely to obtain positive outcomes from SMT.
Background
Pain affecting the spine not only has a significant impact on the individual’s health and functional ability but also carries considerable costs to the economy and society at large, mostly derived from treatment expenses and work absenteeism (1, 2). Back and neck pain combined are the number one cause of years lived with disability and the fourth leading cause of years lost to disability globally (2, 3). At any time, over 11% of the world population suffers from pain in the spine (4, 5). The prevalence has been increasing over the past decade (2), particularly among working-age females in high-income countries (5, 6). Chronic cases where pain lasts for more than 3 months significantly contribute to the increasing burden of spine pain (1, 2). Likewise, pain affecting the spine affects more than 50% of patients with chronic pain (1, 7), a condition whose estimated direct and indirect costs are hundreds of billions of dollars (8). The frequent use of inappropriate and invasive clinical interventions has been suggested as one of the main reasons for this increasing burden (1, 8, 9).
Throughout the past decade, recommendations for the evaluation and treatment of back pain have shifted toward less invasive, non-pharmacologic approaches. This is partly the consequence of the opioid use epidemic in North America, largely driven by high rates and doses of opioid prescriptions for non-cancer pain (10–12). The Lancet series on low back pain (LBP) highlighted an over-reliance on secondary care, imaging, opioids, spinal injections, and surgery (9, 13). Instead, currently available data provide stronger support for the use of conservative interventions and self-management strategies (9, 13–15). This is reflected in the recent publication of systematic reviews and clinical practice guidelines exclusively devoted to summarizing the evidence and recommendations for non-invasive treatments for neck pain (NP) and LBP (16–18). Among these interventions, manual therapy is frequently recommended as one of many front-line options for spine pain (13–19).
Chiropractic is a health care profession concerned with the management of neuromusculoskeletal conditions and, more specifically, disorders affecting the spine (20). Arguably, chiropractors’ area of expertise lies within the field of spine care and in the application of manual therapy (21, 22). Most chiropractic patients seek care for spine-related conditions (23–25). Likewise, people with back pain frequently visit chiropractors in high-income countries (23, 26, 27). Chiropractors strongly rely on the use of manual therapy, particularly spinal manipulation (SM), which is the main form of care they provide (24, 26). In the United States, where data are available, chiropractors perform a large proportion of all SM treatments (28, 29). Chiropractic SM is sometimes referred to as a chiropractic or spinal adjustment in the literature (30). Typically, a spinal adjustment consists of the application of a high-velocity, low-amplitude controlled thrust force to a spinal segment.
The clinical indication of chiropractic adjustment has been the subject of controversy (31). However, provided by chiropractors for spine pain was recently demonstrated to be cost-effective and rarely inappropriate (32, 33). Furthermore, accumulating evidence on the effectiveness of CHIROPRACTIC ADJUSTMENT for the treatment of acute and chronic back and neck pain has rendered it an acceptable management option (8, 27).
Recent research on CHIROPRACTIC ADJUSTMENT suggests that chiropractic care may be evolving from the field of complementary and alternative medicine toward becoming a mainstream option for spine pain (22, 34). However, there is a need to summarize the most up-to-date research in the field for a better understanding of this evolution. Here, we aimed to review the most recent randomized clinical trials on the effectiveness and efficacy of CHIROPRACTIC ADJUSTMENT for the management of NP and LBP, mostly published in the past decade. In addition, recommendations from state-of-the-art clinical practice guidelines will be presented, as well as a perspective on challenges and future directions for research on CHIROPRACTIC ADJUSTMENT and spine pain. While the narrative review will be informed not exclusively by studies where chiropractors apply CHIROPRACTIC ADJUSTMENT, this is done to inform chiropractic clinical practice with the best current available evidence.
Low Back Pain and Chiropractic Adjustment – Research Articles
Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Cochrane Database Syst Rev. 2021 Sep 28;9(9):CD009790.
Pain Med. 2020 Feb 1;21(2):e139-e145.
Coulter ID, Crawford C, Hurwitz EL, Vernon H, Khorsan R, Suttorp Booth M, Herman PM. Spine J. 2018 May;18(5):866-879.
Paige NM, Miake-Lye IM, Booth MS, Beroes JM, Mardian AS, Dougherty P, Branson R, Tang B, Morton SC, Shekelle PG. JAMA. 2017 Apr 11;317(14):1451-1460.
Clar C, Tsertsvadze A, Court R, Hundt GL, Clarke A, Sutcliffe P. Chiropr Man Therap. 2014 Mar 28;22(1):12.
Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW. Cochrane Database Syst Rev. 2011 Feb 16;(2):CD008112.
Cronholm PF, Nicklin DE. Am Fam Physician. 2012 Apr 15;85(8):763-4.
Tettambel M. Am Fam Physician. 2012 Apr 15;85(8):760-2.
Bronfort G. Evid Based Med. 2011 Oct 25.
Bronfort G, Maiers MJ, Evans RL, Schulz CA, Bracha Y, Svendsen KH, Grimm RH Jr, Owens EF Jr, Garvey TA, Transfeldt EE. Spine J. 2011 Jul;11(7):585-98.
Rubinstein SM, van Middelkoop M, Assendelft WJ, de Boer MR, van Tulder MW.
Spine (Phila Pa 1976). 2011 Jun;36(13):E825-46.
Walker BF, French SD, Grant W, Green S.
Spine (Phila Pa 1976). 2011 Feb 1;36(3):230-42.
Leininger B, Bronfort G, Evans R, Reiter T. Phys Med Rehabil Clin N Am. 2011 Feb;22(1):105-25.
Maiers MJ, Westrom KK, Legendre CG, Bronfort G. BMC Health Serv Res. 2010 Oct 29;10:298.
Farabaugh RJ, Dehen MD, Hawk C. J Manipulative Physiol Ther. 2010 Sep;33(7):484-92.
Bronfort G, Haas M, Evans R, Leininger B, Triano J. Chiropr Osteopat. 2010 Feb 25;18:3.
Gay RE, Ilharreborde B, Zhao KD, Berglund LJ, Bronfort G, An KN. Spine J. 2008 Nov-Dec;8(6):982-90.
Lawrence DJ, Meeker W, Branson R, Bronfort G, Cates JR, Haas M, Haneline M, Micozzi M, Updyke W, Mootz R, Triano JJ, Hawk C. J Manipulative Physiol Ther. 2008 Nov-Dec;31(9):659-74.
Paatelma M, Kilpikoski S, Simonen R, Heinonen A, Alen M, Videman T. J Rehabil Med. 2008 Nov;40(10):858-63.
Bronfort G, Haas M, Evans R, Kawchuk G, Dagenais S. Spine J. 2008 Jan-Feb;8(1):213-25.
Liddle SD, Gracey JH, Baxter GD.Man Ther. 2007 Nov;12(4):310-27. Epub 2007 Mar 28. Review.
Chou R, Huffman LH; American Pain Society; American College of Physicians. Ann Intern Med. 2007 Oct 2;147(7):492-504. Review. Erratum in: Ann Intern Med. 2008 Feb 5;148(3):247-8.
Strine TW, Hootman JM. Arthritis Rheum. 2007 May 15;57(4):656-65.
more…
Clarke J, van Tulder M, Blomberg S, de Vet H, van der Heijden G, Bronfort G. Spine (Phila Pa 1976). 2006 Jun 15;31(14):1591-9.
Hurwitz EL, Morgenstern H, Kominski GF, Yu F, Chiang LM. Spine (Phila Pa 1976). 2006 Mar 15;31(6):611-21; discussion 622.
Fritz JM, Childs JD, Flynn TW. BMC Fam Pract. 2005 Jul 14;6(1):29.
Gay RE, Bronfort G, Evans RL. J Manipulative Physiol Ther. 2005 May;28(4):266-73.
Bronfort G, Evans RL, Maiers M, Anderson AV. Manipulative Physiol Ther. 2004 Oct;27(8):503-8.
Haas M, Groupp E, Kraemer DF. Spine J. 2004 Sep-Oct;4(5):574-83.
You might want to think twice before swinging a heavy baseball bat or lifting a heavy suitcase. Unless you’re in tip-top condition, you could be putting yourself at risk of a muscle strain in the lumbar spine.
Reach behind and feel the bumps of your spine, just above the buttocks. This is your lumbar spine. When one or more of the many muscles surrounding the lumbar spine is stretched or torn, it’s called a strain. As you can imagine, when muscle strains occur in this area, they make ordinary, everyday activities involving the low back painful and difficult.
Anyone can suffer a muscle strain, although being active increases people’s risk. Direct trauma to the back, lifting heavy objects and repeated injury to the low back can also make people more prone.
While strains often occur suddenly, they can also develop over time from long-term irritation, such as from poor posture or repeated injury. For that reason, chiropractors classify strains as either acute or chronic. Acute strains usually occur after a single movement, like a sudden twist or bend, and are usually followed immediately by pain. Typically, however, this pain diminishes for a bit and returns later along with stiffness. If the injury didn’t damage the joints or the surrounding tissue, this subsequent pain usually diminishes within a few days.
A chronic strain, on the other hand, develops after people repeatedly tear muscles around the spine. If an acute strain occurs over and over again, for example, it can lead to a chronic strain. Symptoms of chronic strain vary in terms of length and intensity, but usually include a mild, persistent ache in the low back. Many people with the condition also start to modify their daily activities so as to avoid flare-ups.
In either case, your chiropractor can offer effective management. After assessing what caused and contributed to your strain, he or she will determine the most effective way to decrease your pain, improve your muscle function and restore your comfort.
An iliopsoas muscle strain actually involves two muscles in the thigh, the psoas and the iliacus. To understand how they work, think of the roles a pilot and a co-pilot play in the navigation of an airplane. The psoas muscle acts like a pilot, determining the speed and direction of the thigh’s movement, but gives some responsibility to the iliacus muscle, which acts like a co-pilot. As a team, the two muscles work as the chief thigh flexors, helping you raise your knees to your chest.
An iliopsoas muscle strain occurs when muscle fibers or tendons in either the psoas or the iliacus get damaged or torn, which can affect the way all the thigh muscles function. People who suffer from such a condition often complain about an achy pain in the inner part of their thigh. This pain can develop immediately or even up to a day after someone injures either muscle.
The name iliopsoas comes from combining the words psoas and iliacus, as the two muscles actually meet and share a common tendon, which attaches them to the femur (thighbone). For that reason, and because it’s often difficult to tell whether an iliopsoas muscle strain has affected the psoas or the iliacus, chiropractors often refer to them simply as the iliopsoas.
Both muscles are very strong, so generally, those who participate in thigh-intensive sports like hockey and soccer are more susceptible to the condition. Related injuries, like groin strains, can also damage the iliopsoas, especially when the leg is in a vulnerable position.
Other factors that can contribute to an iliopsoas muscle strain include muscle imbalance, which forces one group of muscles to work too hard and fatigue more easily; muscle fatigue, which can occur under excessive stress; previous injuries, which can make the iliopsoas more susceptible if left untreated; and any joint misalignments or dysfunctions in the lumbar spine or pelvis, which can affect how the muscles in the leg function. In addition, quick or misjudged movements, like a slip or fall, can also cause the condition.
Iliopsoas muscle strains range in severity from mild, which only involve a slight tear, to severe, which can involve a large tear and possibly bleeding and swelling. In most cases, mild strains take 2 to 10 days to heal, moderate strains take anywhere from 10 days to 6 weeks to heal and more severe strains take 6 to 10 weeks to heal.
Chiropractic care is effective with most of these strains. Your chiropractor will perform an evaluation to determine what caused the strain and implement a plan of care and rehabilitation program to speed your recovery. With very severe tears, however, patients sometimes require medication and surgery. If so, your chiropractor can explain what this will involve and make a suitable referral
Reach behind you and feel the center of your low back, just above the buttocks. This is your lumbar spine. Lumbar facet irritation is a painful condition affecting the joints in this area, called the lumbar facet joints. These are responsible for connecting the vertebrae (individual bones) in the spine, providing the spine with protection, limiting excessive motion and preventing the vertebrae from locking together.
Patients suffering from lumbar facet irritation usually complain of a well-localized low back pain, meaning they can pinpoint the exact site of discomfort. The condition is closely related to lumbar facet syndrome — however, patients with the latter also feel referred pain in one hip, buttock or upper leg. Facet irritation often precedes facet syndrome, usually if someone hasn’t had his or her irritation treated properly.
The onset of lumbar facet irritation is often sudden, occurring after a misjudged movement or while recovering from a bent position. These activities may stretch the joint capsules (which protect and support the joints) or jam the facet joints, causing subluxations (restricted motion or abnormal positioning) in the spine and painful swelling. Other causes include poor posture, everyday wear-and-tear and trauma to the low back.
Symptoms of facet irritation usually get worse when people sleep on their stomach, work with their arms above their head or rise from a sitting position. All these activities expose the joints to stress that they aren’t accustomed to, making them more vulnerable to injury and irritation.
Chiropractic care is effective for lumbar facet irritation. Chiropractors perform a procedure called spinal manipulative therapy, also known as an adjustment, which relieves pain and restores function to misaligned or malfunctioning joints.
Reach behind you and feel the center of your low back, just above the buttocks. This is your lumbar spine. Lumbar facet syndrome is a painful condition affecting the joints in this area, called the lumbar facet joints. These are responsible for connecting the vertebrae (spinal bones) in the spine, providing it with protection, limiting excessive motion and preventing the vertebrae from locking together.
Patients suffering from lumbar facet syndrome usually complain of a well-localized pain in the lumbar spine, as well as a duller type pain in one hip, buttock or upper leg. This irritation is called referred pain, which is a type of pain that originates in one area and spreads to surrounding areas.
Symptoms of facet syndrome usually get worse when people sleep on their stomach, twist their torso, work with their arms above their head, extend backward or rise from a sitting position. All these activities expose the joints to stress that they aren’t accustomed to, making them more vulnerable to injury and irritation.
Such problems usually begin after patients have a similar condition called lumbar facet irritation and don’t get proper care. This condition usually develops suddenly, sometimes after a misjudged movement involving the back, like sudden twisting, or while people are recovering from a bent position. It can also be the result of repetitive twisting movements like swinging a golf club. These activities stretch joint capsules (which protect and support the joints) or jam facet joints, leading to painful swelling and inflammation. Other causes of facet irritation include subluxations (stuck or misaligned joints), poor posture, everyday wear-and-tear and trauma to the low back.
The difference between lumbar facet syndrome and lumbar facet irritation is that patients with the latter only have pain in the low back, and not the accompanying referred pain. For either condition, chiropractic care is an effective plan of management. Chiropractors perform a procedure called spinal manipulative therapy, also known as an adjustment, which relieves pain and restores function to misaligned or malfunctioning joints.
Vertebral subluxation complex (VSC), which chiropractors often refer to simply as a subluxation, is a fitting title for a condition that is extremely complex. There are five recognized components that contribute to this condition. To further its complexity, patients may not be aware that they have a problem because, initially, subluxations may not cause pain or discomfort.
Let’s take a step back to see where VSC of the lumbar spine occurs. The lumbar makes up the bottom of the spine, starting at your low back and ending just above your buttocks. It’s below the thoracic spine, which makes up the mid back, and the cervical spine, which makes up the neck.
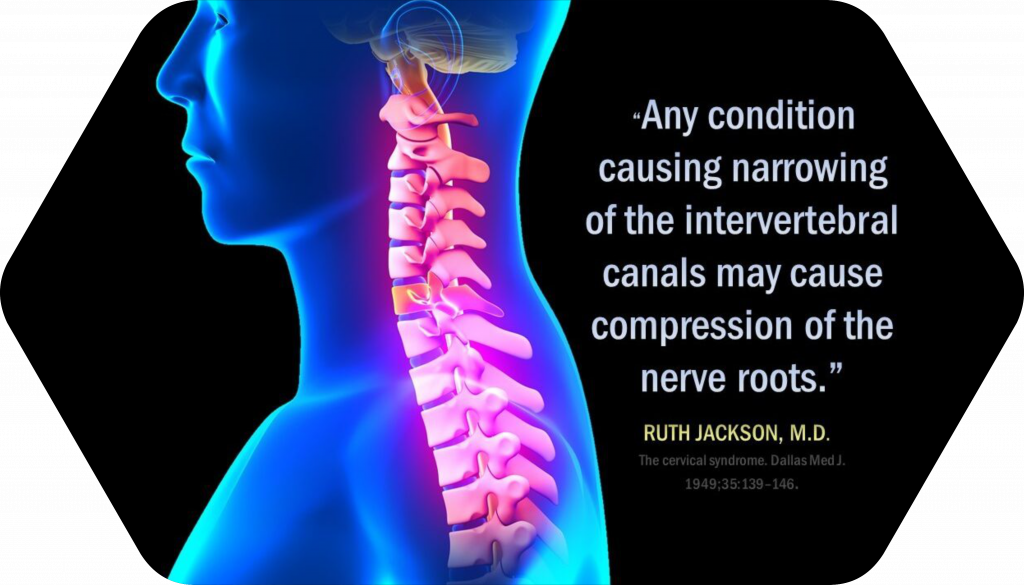
VSC in the lumbar spine occurs when vertebrae in the low back lose their normal motion or position, which can lead to local inflammation and affect the delicate nerves in the spinal cord that carry messages between the brain and the rest of the body.
These nerves, along with the brain, collectively make up the central nervous system. The nerves leave the spinal column through holes, formed between vertebral joints, and branch off and control the health and function of every cell, tissue and organ.
Research suggests that subluxations affect how these parts function by interfering with the brain-body communication system. Imagine a healthy nervous system surrounded by clean water, and the interference as muddy and murky water that starts to pollute it.
A variety of external and internal factors can cause subluxations. Since chiropractic’s inception, trauma, toxins and emotional stress have been identified as the primary causes of subluxation. Traumatic causes include car accidents and falls, chemical toxins include alcohol, drugs and environmental pollutants, and emotional stress includes everyday problems like worrying and anxiety.
When any of these is present, it can lead to the beginning of VSC, and possibly the entire five components of the condition. The first stage is kinesiopathology, which begins when spinal joints become stuck, forcing the joints around them to work harder in order to compensate. Unfortunately, this compensation does not change the fact that the spinal joints aren’t functioning properly, and thus the spine’s normal curvature can distort and the stuck joints can contribute to nerve irritation.
Most often, this occurs when malfunctioning spinal bones stretch, twist or pull nerve tissue. When this is serious enough it can lead to neuropathology, the second stage of VSC, which can involve either extreme nerve irritation or a pinched nerve. Pinched nerves, which are quite rare, can produce feelings patients frequently describe as “pins and needles” or a numb sensation surrounding and even far from the spine. Irritated nerves can affect the parts of the body they communicate with and increase a person’s susceptibility to disease.
This interference in the nervous system can lead to the third component of VSC, myopathology, which involves abnormal muscle function. With myopathology, nerve impulses can diminish to the point that they under-stimulate muscles, which causes muscles to weaken and atrophy; or, they can become too strong and over-stimulate muscles, which causes muscles to work too hard and tighten, to become strained and potentially to go into spasm. Either of these problems can lead to inflammation in muscles and joints, which can cause further complications by spreading to the rest of the soft tissues in the spine. If that happens, it can lead to the fourth stage of VSC, histopathology, which involves abnormal function of soft tissue. This occurs when abnormal spinal joint function diminishes blood supply and leads to long-term swelling of structures like ligaments, disks and other soft tissues.
If people don’t seek care during any of these stages, VSC can affect the whole body. This is pathophysiology, the fifth and final stage of VSC, when degenerative changes in the spine begin to spread. At this stage, calcium deposits may have built up, and are eventually recognizable as bone spurs and other abnormal growths. When this happens, your body has gone to the extreme of compensating for a malfunctioning or traumatized joint by actually creating a growth reminiscent of new bone. It has slowly transformed immobile, untreated joints into solid blocks of calcium. Known as subluxation degeneration, this final component of VSC becomes more common as people get older.
While it takes many years for someone to develop problems associated with the final component of VSC, the condition can begin at any age. That’s why it’s important to visit your chiropractor, as he or she can check for subluxations and provide you with ideal care. Your chiropractor will use an adjustment to correct your subluxations, which involves a high-speed thrust that realigns faulty joints and allows the body to heal. Combined with proper spinal care, this can prevent VSC from progressing into a more serious condition.
Almost everyone experiences low back pain. To alleviate it, the key is identifying which of the many conditions that affect the back is responsible.
Lumbar disk herniation is a well-known cause of back pain, but it’s not as common as most people think. In fact, only about 5% of those who go to the doctor for low back pain have a disk herniation.
These people usually experience back and leg pain, as well as muscle spasms in their low back and leg. They also commonly report muscle weakness, numbness and pins and needles in the thigh, leg and foot.
As herniations usually occur on one side of a disk, the pain is generally worse on the corresponding side of the back. The pain can worsen with coughing, straining or sneezing, as well as slouching and bending, which compresses irritated disks in the spine. It often gets better with bending backward or leaning to one side (the one opposite to the pain), which takes pressure off irritated disks. Because of this, people with lumbar disk herniation often adopt a particular posture or walking stance to ease discomfort — bent sideways and forward, or with their knees slightly bent to relieve pain in the legs.
While the pain of lumbar disk herniation can radiate into one or both legs, the cause of the condition occurs in the lumbar spine, which is just above your buttocks. Your spine comprises bones called vertebrae, and in the lumbar spine there are five. Like the coils of a slinky, these vertebrae are stacked one on top of the other and move in unison.
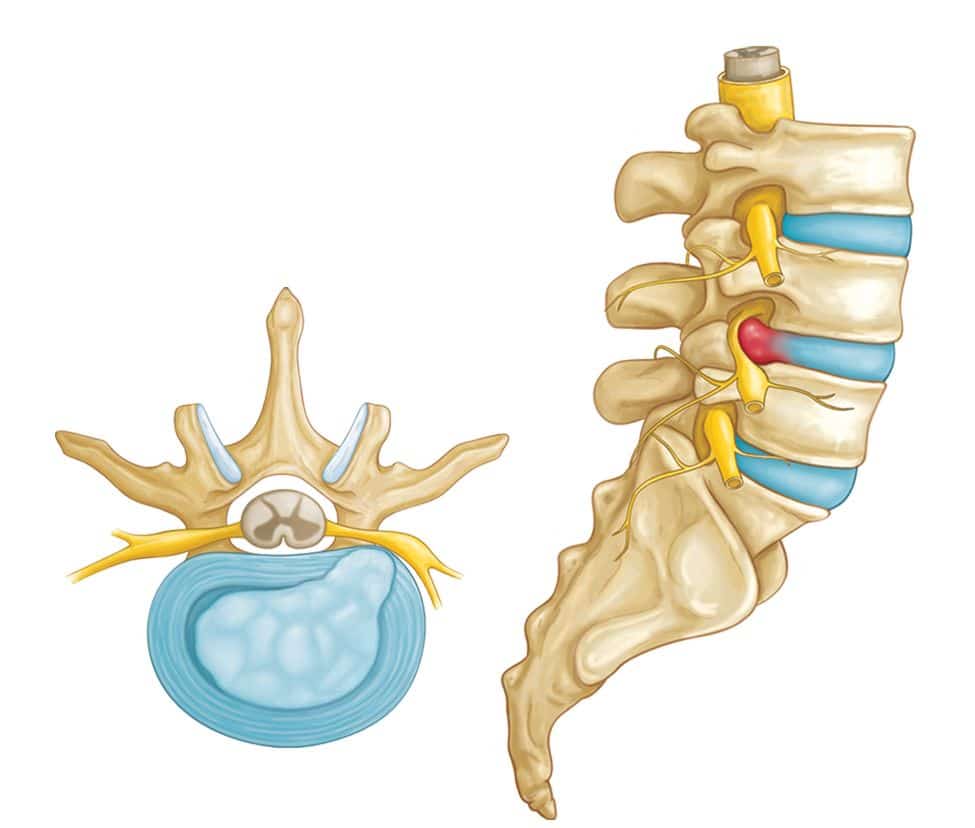
To prevent friction during this movement, intervertebral disks cushion and protect the vertebrae. These disks are soft, fluid-filled pads, and when they become herniated, the gel-like material inside bulges out into the spinal canal (usually more to one side or the other than straight back).
Within the spinal canal lies the spinal cord, which contains spinal nerves that exit between vertebrae and branch out to the rest of the body. The displaced gel compresses these nerves, causing pain in the low back and the areas of the body to which nerves travel from the spinal cord. In severe cases, the displaced gel can even compress the spinal cord itself, and in such cases, chiropractors usually refer patients to a medical doctor or a hospital.
Usually, a single event doesn’t trigger such a herniation. A disk herniation is more likely a result of steady abuse. People whose work involves lots of twisting, bending, sitting or heavy lifting are more at risk, as these activities cause disk stress and wear and tear. Truck drivers, for example, endure prolonged periods of sitting in a vibrating vehicle, which can cause tremendous stress for the intervertebral disks and over time lead to a herniation.
While extreme cases of this condition may require surgery, conservative chiropractic care is usually sufficient. For that reason, people with lumbar disk herniation should consult their chiropractor to discuss methods of care that can relieve pressure on affected disks and ease associated muscle spasms and inflammation.
Almost every movement you perform involves your joints. Walking, running, typing and lifting are just a few of the common things people do that would be impossible without them. To prevent our bones from wearing down during these movements, our joints rely on cartilage, a spongy tissue that helps to cushion the friction between connecting bones. Without it, everyday activities would be painful.
Osteoarthritis (OA) is a degenerative joint disease that causes this cartilage to break down and become rough and flaky, making movement in the affected area difficult. OA usually occurs in weight-bearing joints, like the hips or the knees, which support the body. However, any joint can become affected. In fact, OA can occur in several joints at the same time. It’s possible, for example, to have pain in one knee and not the other, and at the same time have pain in the shoulder or the ankle.
Patients with OA often report having mild pain, morning stiffness and limited movement in the affected joint. The pain tends to come in bouts, with particularly painful periods followed by periods of relief. Patients usually report the most discomfort at night and after extensive use of the affected joint. Although rare, some patients also complain of a complete loss of motion in certain areas.
No one knows for sure what causes OA, but age and obesity seem to play a role. Almost everyone experiences some changes in their joints by the age of 40, and although few people show any symptoms, OA occurs most often in those who are middle-aged and older. Obesity also increases the risk of becoming affected as extra weight puts more stress on joints.
While there’s no cure for OA, your chiropractor can implement a management plan that prevents its progression, promotes joint health and relieves pain. By seeing your chiropractor and adopting lifestyle changes, you can reduce the condition’s debilitating effects.
Schedule An Appointment
If you suffer from joint pain please contact our office to schedule an appointment with one of our chiropractors today. One of our qualified professionals will perform a comprehensive physical exam to determine the best treatment options available to you. We will gladly answer any of your questions.